
Protein Supplements For Weight Management? Do I Need Them And Why?
Sorry, it's just marketing 😒

The media has told us a protein meal replacement is a good way to target weight management without additional carbs or fats that other foods can provide. Is this true or just marketing?
Protein meal replacement = Protein powder + fibre + vitamins + rubbish + marketing
Meal Replacements vs Protein Shakes
Meal Replacement Shakes Intended to substitute one or two meals of your daily diet.
They are usually fortified with vitamins and minerals and offer more fibre, carbohydrates, and calories per serving than a protein shake, although they are lower in calories than actual meals. they also provide protein, but at lower levels than most protein shakes.
Protein Shakes Intended to supplement a regular diet, not to replace a meal.
They are to be consumed before or after a workout with typically up to 25 g of protein per serving and usually have less than 5 g of carbohydrates since they are not intended to be full meals while Tend not to contain any added vitamins and minerals other than those provided by the protein source.

Myprotein Protein Meal Replacement Blend Explained
- Skimmed Milk Powder (just drink Skimmed Milk).
- Dietary Fat Concentrate from Refined Coconut Oil, Refined Soybean Oil (why do you need oils? you don’t) .
- Milk Proteins, Whey Powder from Milk (This is just Whey Protein).
- Maltodextrin, Emulsifier (to make it thicker and last longer).
- Stabiliser (Triphosphates).
- Antioxidants (Fatty Acid Esters of Ascorbic Acid, Alpha-Tocopherol) — commonly used as a flour improver.
- Anti Caking Agent (Calcium Phosphates) — essentially is Talc, used in many different food products to prevent clumping.
- Whey Protein Concentrate (Milk, Soy Protein Isolate)— again just get Whey Protein or Soy Protein, no need to get both
- Flavouring — OK
- Inulin Powder (Inulin has no calories and can function as a fat substitute in margarine and salad dressings. In baked goods, it may be used to add fibre and can substitute for some flour without affecting the taste and texture) — Its fibre.
- Potassium Citrate — pH buffer, which contributes to its use as a preservative.
- Thickener (Xanthan Gum) ,
- Potassium Phosphate Powder (imitation dairy creamers, It functions as an emulsifier, stabilizer and texturizer)
- Salt
- Calcium Chloride (It is used in salt processing to add a salty taste to pickles and other foods without increasing sodium content it also increases firmness and shelf life.)
- Sweetener (Sucralose) — A terrible choice of sweetener being artificial vs stevia being naturally derived sweetener from the stevia plant,
- Vitamin and Mineral Premix (Folic Acid, Vitamin C, Niacin, Iron, Vitamin E, Zinc, Pantothenic Acid, Fluoride, Manganese, Vitamin B6, Vitamin B2, Vitamin B1, Copper, Vitamin A, Iodine, Vitamin K, Selenium, Molybdenum, Biotin, Chromium, Vitamin D, Vitamin B12)
- Magnesium Oxide (a food additive for powdered foods desiccant (drying agent), colour retention, pH modification or as a magnesium mineral supplement)
You can start to see a picture of the balance between convenience (marketing) and “what am I putting in my body?“
Conventional thinking will say that “Protein and Meal Replacement shakes are not meant to replace a meal. Their role is to supplement your diet and make it easier to meet your daily protein requirements when you're active”, the keywords here are “replace” and “active”.
What “replace“ means in this context is not stop eating normal food that contains protein such as lean meats, poultry, fish and seafood, eggs, eggs, nuts and legumes and beans and replace them for protein powder. However, generally speaking, while the list above includes more completes type of protein a protein is a protein and while I don’t recommend long term protein powder replacement, in a simplistic point of view and from the body point a protein is a protein.
What “active” means in this context is obviously doing exercise, now you don’t necessarily have to exercise to manage your weight.
A gram of carbohydrate contains 4 calories. A gram of protein also contains 4 calories. A gram of fat contains 9 calories. With this in mind, you can start thinking about “calories in versus calories out”
The calories in versus calories out is a model is based on the idea that to maintain a stable weight, the number of calories you eat needs to match the number you expend. “Calories in” refers to the calories you get from the foods you eat, while “calories out” is the number of calories you burn
The main difference is how the protein and the additional protein will affect your body. A 2008 paper published in The American Journal of Clinical Nutrition by Douglas Paddon-Jones and colleagues states
“protein generally increases satiety to a greater extent than carbohydrate or fat and may facilitate a reduction in energy consumption under ad libitum dietary conditions, higher-protein diets are associated with increased thermogenesis, which also influences satiety and augments energy expenditure and maintenance or accretion of fat-free mass—in some individuals, a moderately higher protein diet may provide a stimulatory effect on muscle protein anabolism, favouring the retention of lean muscle mass while improving metabolic profile”
What should I take then?
Not a Meal Replacement as stated before, in fact, you should look at your average macronutrient intake and see if and how much more protein you need which depends on your physical activity and age.
As a Protein intake analysis of the National Health and Nutrition Examination Survey from 2001–2014 by Claire E Berryman and associates concludes
The majority of the US population exceeds minimum recommendations for protein intake. Protein intake remains well below the upper end of the AMDR (Acceptable Macronutrient Distribution Range), indicating that protein intake, as a percentage of energy intake, is not excessive in the American diet.
When looking into Protein intake for different populations we start to see how starting at 40 we should increase our intake. as Kristi Wempen, a Mayo Clinic Health System registered dietitian nutritionist comments
Once you hit 40-50 years old, sarcopenia starts to set in, which means you start losing muscle mass as you age, to help prevent this and to maintain independence and quality of life, your protein needs increase to about 1 gram per kilogram of body weight.
People who exercise regularly also have higher needs, about 1.1-1.5 grams per kilogram. People who lift weights regularly or are training for a running or cycling event need 1.2-1.7 grams per kilogram.Excessive protein intake would be more than 2 grams per kilogram of body weight each day.
If you are overweight, your weight is adjusted before calculating your protein needs in order to avoid overestimating,” says Wempen. “You can see a dietitian to help develop a personalized plan.
In another study, Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People From the PROT-AGE Study Group,. Jürgen Bauer MD and associates found
To maintain physical function, older people need more dietary protein than do younger people; older people should consume an average daily intake at least in the range of 1.0 to 1.2 g/kg BW/d.
Most older adults who have an acute or chronic disease need even more dietary protein (ie, 1.2–1.5 g/kg BW/d); people with severe illness or injury or with marked malnutrition may need as much as 2.0 g/kg BW/d.
Older people with severe kidney disease who are not on dialysis (ie, estimated GFR < 30 mL/min/1.73m2) are an exception to the high-protein rule; these individuals need to limit protein intake.
Protein quality, timing of intake, and amino acid supplementation may be considered so as to achieve the greatest benefits from protein intake, but further studies are needed to make explicit recommendations.
In combination with increased protein intake, exercise is recommended at individualized levels that are safe and tolerated.
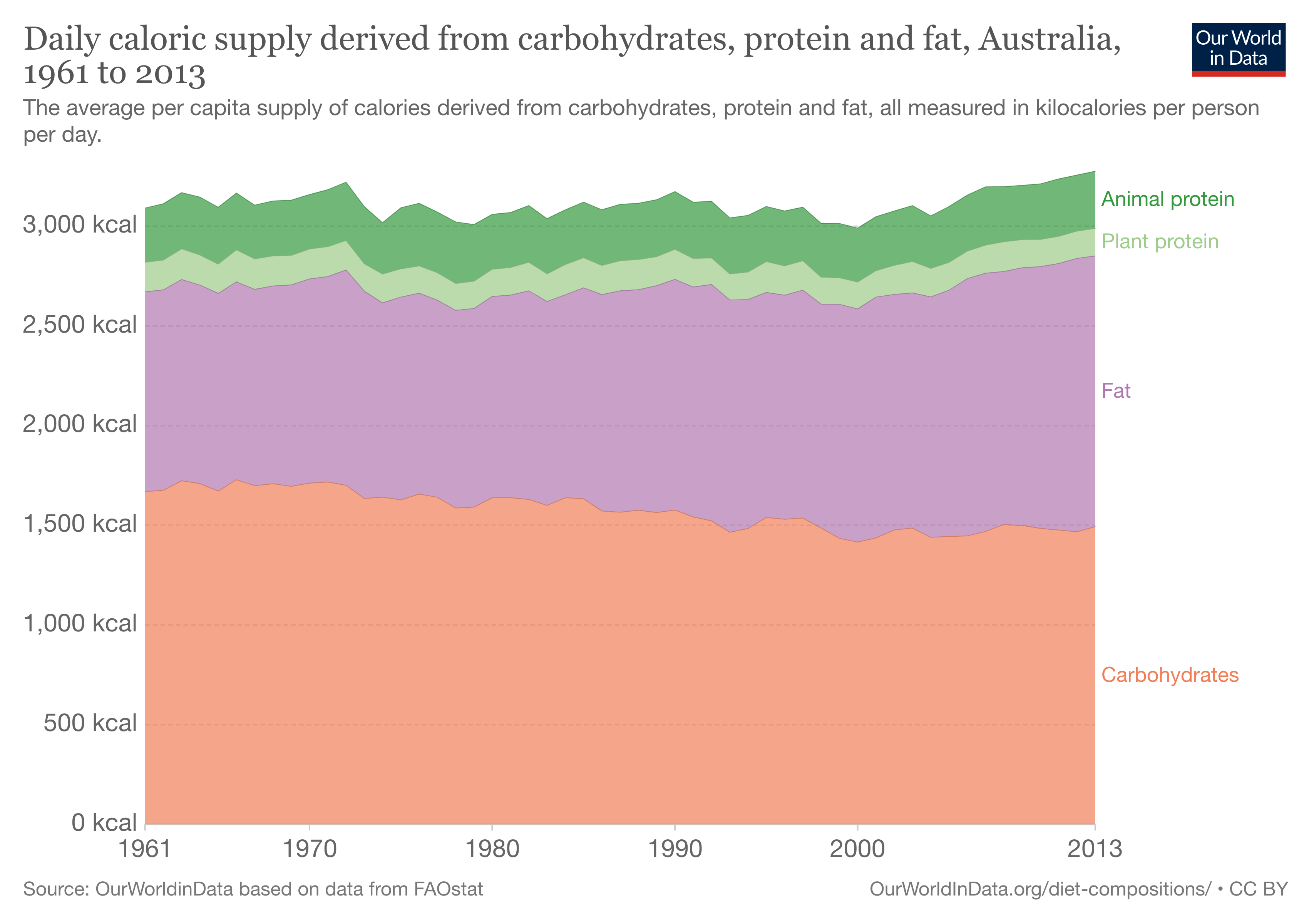
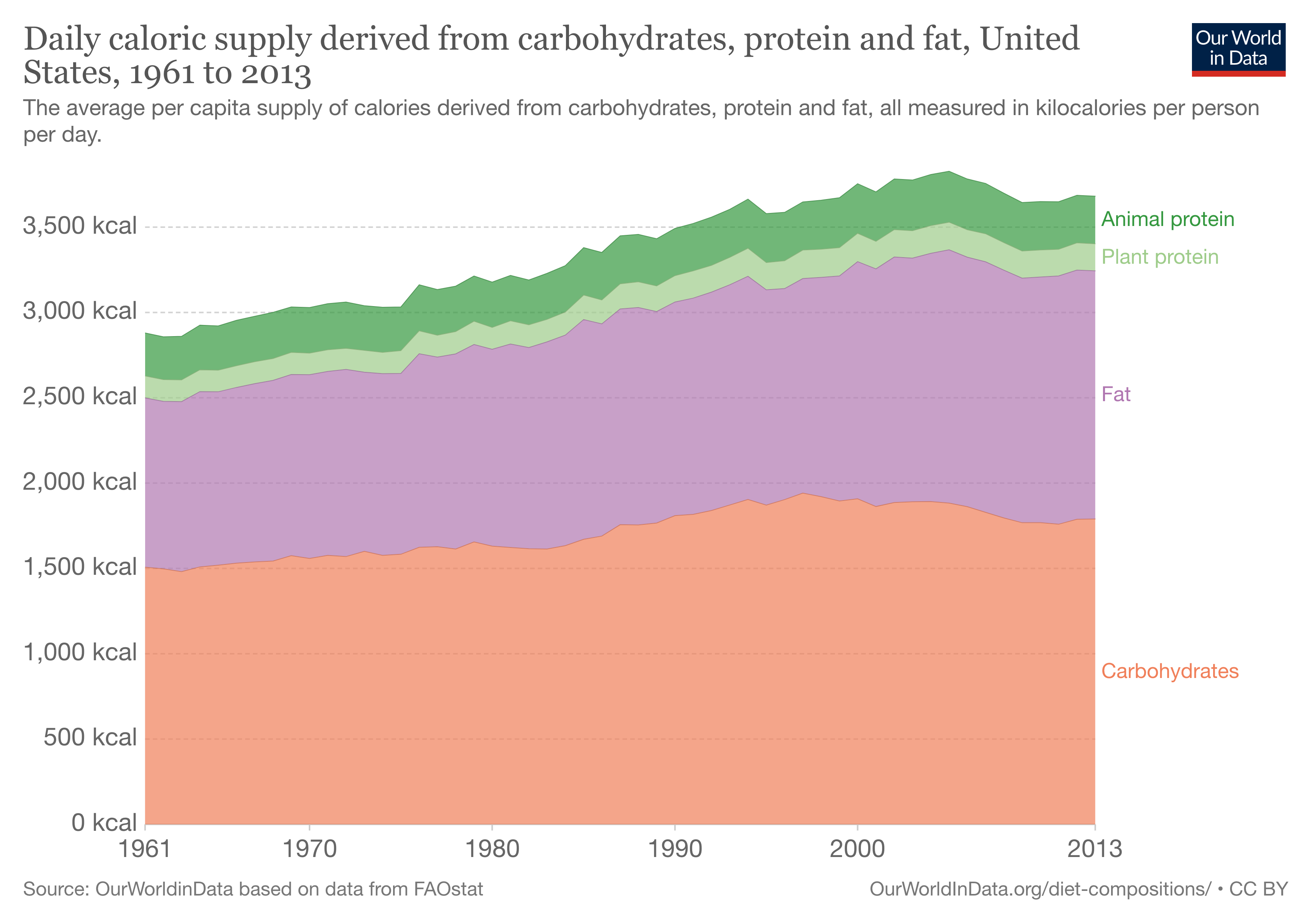
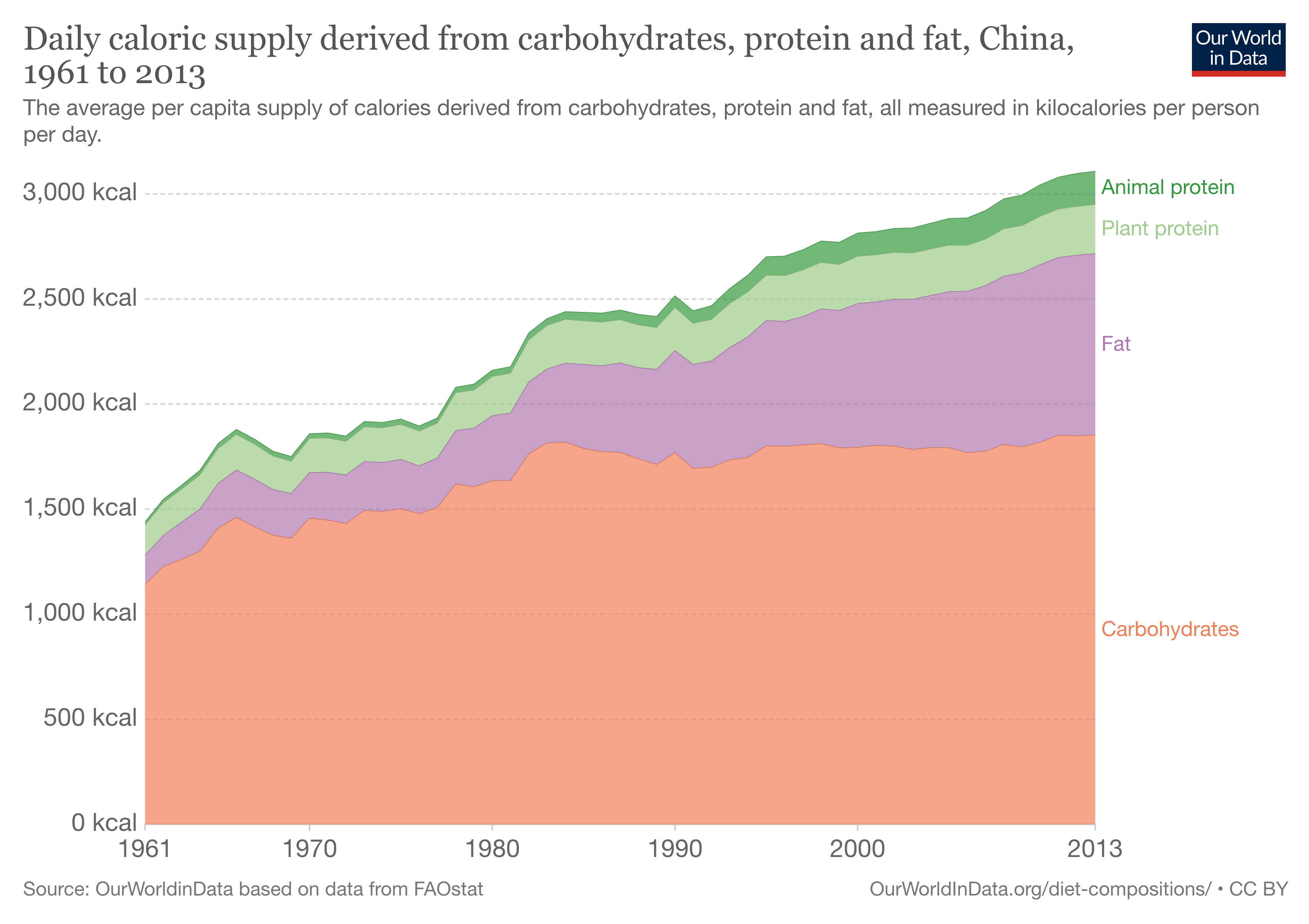
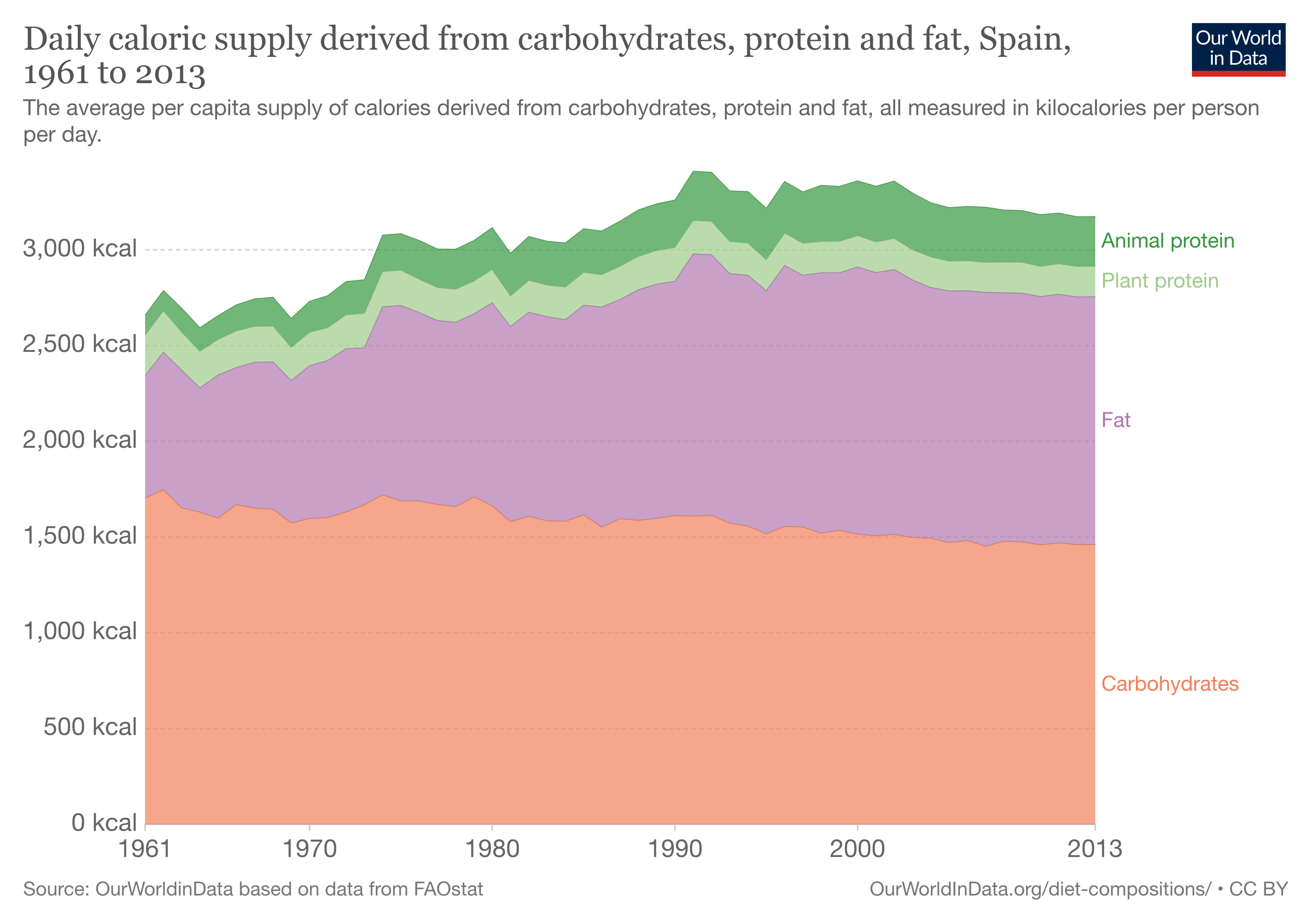
What’s the big picture?
Here’s the most recent data on macronutrient intake trends from 1962 to 2013 from Australia, the U.S., China and Spain. It is interesting to see the carbohydrates and fat ratio and plant vs animal protein (especially in China)
What’s the alternative?
Instead just add protein powder + fibre (oatmeal, flaxseed, psyllium husk or barley). Insoluble fibre (wheat bran, seeds…) or a ready-made Fiber Supplement + a Multivitamin
What protein powder should i take?
Whey or Pea protein.
Whey protein comes from milk and contains two kinds of protein: whey and casein
During the day: use Isolate or Concentrate protein (Concentrate is usually available in your supermarket)
Before bed: Casein protein
Concentrate protein: Most inexpensive and the most basic and least processed form of whey
Whey Isolate protein: is lower in fat and carbs than Concentrate and better for lactose sensitivities, while is further processed in such a way that much of the carbohydrates and fat are removed
Casein protein: When you add acid or enzymes to milk, it separates out the whey from the casein. About 80 per cent of the protein is casein, which is used to make cheese. Casein is well known as a “time-release” protein because of its slow absorption rate in the gut. This means that it feeds your cells with amino acids at a low level over a long period of time
There are also alternative vegan options that can include pea, flax, quinoa, pumpkin seed, rice and chia seed proteins (often separately), being pea protein is the most popular.
Further considerations and what happens after 40
Sarcopenia Myopenia and Dynapenia: the muscle killers
Sarcopenia is a type of muscle loss (muscle atrophy) that occurs with aging and/or immobility. It is characterized by the degenerative loss of skeletal muscle mass, quality, and strength. The rate of muscle loss is dependent on exercise level, co-morbidities, nutrition and other factors.
Beginning as early as the 4th decade of life, evidence suggests that skeletal muscle mass and skeletal muscle strength decline in a linear fashion, with up to 50% of mass being lost by the 8th decade of life.
Myopenia is a clinically relevant degree of muscle wasting that is associated either with impaired functional capacity and/or with increased risk of morbidity or mortality. The precise cut-points to define the presence of myopenia may be specific to a particular disease or condition and indicates the presence of clinically relevant muscle wasting due to any illness and at any age.
Dynapenia is the loss of muscular strength not caused by a neurological or muscular disease that typically is associated with older adults. Dynapenia is the loss of muscle strength, rather than muscle mass. Possible biological contributors to dynapenia include the nervous system's deteriorating control of voluntary skeletal muscle activation and a decreased number of functioning motor units. The nervous system's lowered ability to stimulate a full muscle contraction subsequently leads to loss of muscle strength and power
What is this means to me?
In the 2015 paper titled Sarcopenia Is Associated With Incident Disability, Institutionalization, and Mortality in Community-Dwelling Older Men by Vasant Hirani MSc, RD, PhD and associates shows
Of the 1705 participants aged 70 years or older, 103 (11.3%) men had incident Activities of daily living disability, 191 (11.2%) men were institutionalized, and 535 (31.9%) had died. At baseline, 14.2% had sarcopenia I, 5.3% had sarcopenia II, and 3.7% had sarcopenia III. Fully adjusted analysis showed that sarcopenia I, II, and III were associated with increased risk of disability, institutionalization, and mortality.
What can I do?

More specifically looking at Sarcopenia due to the risk associated after 40, the primary treatment for sarcopenia is exercise, specifically resistance training or strength training. These activities increase muscle strength and endurance using weights or resistance bands. Moreover, the Society for Sarcopenia, Cachexia, and Wasting developed nutritional recommendations for the management of sarcopenia. They suggest that older adults consume 1.0 to 1.5 g of protein/kg of body weight/d, and include leucine-enriched essential amino acids to the diet (chicken, beef, pork, fish (tuna), tofu, canned beans, milk, cheese, squash seeds, and eggs)
Besides your genetic predisposition, Charles Eugster (on the photo above), is a 96-year-old runner, rower, wakeboarder, body-builder, public speaker and writer, told Vice magazine
I was 87 and realized my body was deteriorating. I had a muffin-top waist and my muscles were getting weaker and weaker. I felt so old. But because I was so vain, I didn't like the idea of it at all. So I joined a body-building gym and employed a personal trainer who was a Mr. Universe to rebuild my body from scratch.
If Charles started at 87, what’s your excuse?
Thanks for reading my blog. Subscribe to get 1 actionable insight to improve your mental or physical health backed by medical research, every Saturday.



